Can exercise training improve maximal aerobic power (VO2max) in children: a meta-analytic review |
JEPonline
Journal of
Exercise PhysiologyonlineISSN 1097-9751
An International Electronic
Journal for Exercise PhysiologistsVolume 2 Number 3 July 1999
Review: Speical Populations-Pediatric
Can exercise training improve maximal aerobic power (VO2max) in children: a meta-analytic reviewLINDA M. LeMURA1 , SERGE P. von DULLIVARD2 , RICHELLE CARLONAS1 and JOSEPH ANDREACCI1
1Division of Exercise Science, Bloomsburg University, Bloomsburg, PA and the 2Human Performance Laboratory, Department of Physical Education and Exercise Science, University of North Dakota, Grand Forks, ND
LINDA M. LeMURA, SERGE P. von DULIVARD, RICHELLE CARLONAS, and JOSEPH ANDREACCI. Can exercise training improve maximal aerobic power (VO2max) in children: A meta-analytic review. JEPonlineVol 2 No 3, 2(3):1-22, 1999. This study was conducted to quantitatively examine the effects of physical training on maximal aerobic power (VO2max) in children using the meta-analytic technique. In addition, we examined the effects of experimental design, training protocol, gender, age, and testing procedures on the VO2max of children. Past research used in the analyses were delimited to studies examining the effects of various forms of muscular strength and endurance training in children <13 years, resulting in a total of 91 studies. However, as numerous studies failed to provide sufficient information or adequate statistics, the final pool of research was confined to 20 studies with 32 effect sizes (ES), totaling 562 subjects. Studies which utilized a control group generated a mean pre-post training ES of 1.1± 0.1, compared to a mean ES of 0.32± 0.2 from those in which subjects served as their own controls (p<0.0009). Studies that were cross sectional (XS) typically reported a higher VO2max in the trained group (ES=1.7± 0.3) compared to pre-to-post test designs (ES = 0.63± 0.6). Analyses of the subjects characteristics indicated that children in the 8 to 10 year old (ES=0.47± 0.4) range were trainable; however not nearly to the same extent as their 11 to 13 year old counterparts (ES=1.1± 0.7, p<0.02). The mean ES for girls and boys was 1.0± 0.6 and 0.64± 0.9, respectively. An analysis of investigations which utilized a sufficiently intense training stimulus, vs. an inadequate training stimulus, resulted in significant improvements in VO2max after training (ES=0.33± 0.2 vs. ES=1.2± 0.5, p<0.0004). Children improved their VO2max by an average of 6.0% (47.1± 4.3 versus 50.1± 4.6) after training. The results of this quantitative review indicate that children are indeed trainable, but the changes in VO2max are modest and are significantly impacted by the experimental design of the investigation, the age of the children, and the nature of training stimulus.
Key words: Meta-analysis, Pediatric, Cardiorespiratory Endurance
INTRODUCTION
The manner in which physical training induces physiologic, metabolic, anatomic and hemodynamic changes in adults has been thoroughly researched. Although the mechanisms by which these alterations are accomplished remain the focus of investigation and debate, it is clear that training enhances cardiovascular function through quantifiable changes in maximal aerobic power (VO2max). During maximal exercise, VO2max is augmented by significant increases in cardiac output (Q) and the arteriovenous oxygen difference (a-vO2diff). These responses are modulated by numerous variables, including a sufficient intensity, frequency, and duration of exercise.Our present understanding of how a child's cardiovascular system responds to physical training continues to be a subject of great interest to investigators because it is unclear how their responses compare with adults. For example, it is known that in adults Q increases proportionately to oxygen consumption (VO2) demands during exercise and that the initial increase in Q is accompanied by increases in the heart rate (HR) and in stroke volume (SV). Children compared to adults demonstrate a lower absolute Q at a given submaximal workload resulting from a dampened increase in SV (1-3). The increases in HR at the commencement of exercise may be attributed to the withdrawal of parasympathetic nervous activity and an increase in sympathetic nervous activity. It is also clear that the SV increases up to an intensity of exercise that is equivalent to 50 to 60% VO2max, after which it begins to plateau, owing all subsequent increases in Q to continual increases in the HR. It is also clear that with increased exercise intensity, systolic and mean blood pressures rise, while systemic vascular resistance may decrease and diastolic blood pressure remains essentially unchanged. Although these cardiovascular alterations are also found in children, whether children are able to improve their fitness similar to adults, as demonstrated by quantifiable improvements in VO2max, continues to intrigue researchers.
The critical stage in physical maturity during which physical training exerts its greatest influence on VO2max remains speculative. For example, early studies by Mirwald et al. (4) and Kobayashi et al (5) found that in longitudinal studies of males, training did not significantly alter VO2max before the age of 12 years. Similarly, Katch (6) explained numerous prerequisite physiological phenomena as integral to any enhancement in VO2max in children. His trigger hypothesis suggested that a maturation of the neuromuscular system, increases in various hormone concentrations and an increase in the lean-to-fat tissue ratio are all necessary precursors to any significant metabolic adaptations in children after training. The critical time in which these maturational events occur are immediately prior to the onset of puberty. Accordingly, any physical training that occurs before that critical period will result in minimal or nonexistent alterations in VO2max. Two subsequent reviews provided by Borms (7) and Bar-Or (8) provided additional support for the contention that exercise training does not significantly enhance aerobic power in children. In the first review, it was noted that the positive effects of training on VO2max is not consistently shown in children, while the second review concluded that VO2max would be changed minimally or not at all after training. In summary, both reviewers suggested that whether or not prepubescent children could demonstrate substantive gains in aerobic power remained uncertain.
In contrast, other studies have reported significant improvements in VO2max as a direct result of engaging in physical training. Investigations by Eisenman and Golding (9) , Mayers and Gutin, (10) , Rowland (11) , and Vaccaro and Mahon (12) indicated that aerobic power can be appreciably altered after training in children, provided a sufficient training stimulus for intensity, frequency and duration exists. Other reviews conducted by Pate and Ward (13) and Sady (14) suggested that children may demonstrate positive adaptations to physical training; however, the responses may be quantitatively and qualitatively less than adults. Sady (14) concluded that a definitive statement concerning the cardiorespiratory effects of training could not be made since few carefully controlled and well-defined training studies including cardiorespiratory variables have been conducted. All these conflicting data leave the question of whether children can improve aerobic power unresolved.
The issue of the aerobic trainability of children is highly significant, since an understanding of it and how these physiologic and metabolic alterations occur could provide insight into the mechanisms for improvement of fitness at all ages.
Endurance fitness improves progressively throughout childhood and adolescence, more so in males compared to females. Studies in adult subjects have demonstrated that VO2max and reduction in O2 requirements at submaximal workloads are strong predictors of endurance fitness. These measures could also play important roles in the development of endurance capacity in the pediatric population. Body mass has been related to VO2max in numerous studies and has been used extensively for determination of intraindividual comparisons of aerobic capacity (15). However, several pediatric studies have reported that VO2max is not well related to endurance fitness in children compared to adults (16, 17). Furthermore, the use of exercise as a rehabilitative model in children with cardiac and pulmonary diseases would be significantly enhanced if improvements in aerobic power could be documented after training. Finally, an understanding of the nature of cardiovascular adaptations to physical exercise would inevitably result in designing safe and effective exercise programs to guide the training of young athletes.
Although there is considerable research to date on the topic of the trainability of children, the issue remains unclear in large part due to the confounding factors of the maturation of children and the methodological design employed by individual researchers. Many studies reporting significant increases in VO2max have been cross-sectional; therefore, the effects of growth and development may have masked the true contribution of training. Clearly longitudinal data are preferential in order to identify the relative contribution of maturation on the development of aerobic power. However, even longitudinal studies will be effected by the methods of training (intensity, frequency and duration) and testing (ergometry vs. treadmill) of young children. Moreover, the presence of matched control subjects will obviously have a tremendous impact on the outcomes of the research. Finally, due to the paucity of studies examining the effects of training in girls, it is unclear if the maximal aerobic responses of girls differ to those of boys. Thus, this quantitative review will examine, utilizing the meta-analytic technique, the effects of physical training, methodological issues, and subject characteristics on VO2max in children.
METHODS
Glass et al. (18) originally developed the statistical technique of meta-analysis in 1977. A meta-analysis on a given research topic is directed toward the quantitative integration of findings from various studies. Each study serves as the unit of analysis; the findings between studies are compared by transforming the results to a common metric called an effect size (ES). Although this review technique provides a quantitative method of combining ES magnitude across studies, it has not been without criticism. The most severe criticism addresses the combination of findings from studies representing different measurement scales, methodologies, and experimental designs. However, the mixing of apples and oranges argument has been addressed by Hedges and Olkin (19) who have revised and extended the original work of Glass (12). Specifically, statistical formulae have been provided (e.g. unbiased ES estimators) that, if used appropriately, will result in a valid and reliable means to combine effects across numerous studies.In this review, the meta-analysis was focused on the specific problem of attempting to elucidate the question of whether physical training can improve VO2max in children. The ongoing debate in the literature indicates that the issue remains unresolved. Therefore, the purposes of this quantitative review were to: (1) locate exercise training studies that utilized children as subjects; (2) identify the effects of the training stimulus on the presence and magnitude of changes in VO2max (3) determine the effect of methodological design on the presence and magnitude of changes in VO2max; (4) identify the impact of gender differences on VO2max; (5) determine the impact of testing methods on VO2max, and (6) provide recommendations for additional studies since the meta-analytic technique highlights potential gaps in the research literature that might be suitable for future investigation.
Selection of Studies
Studies were located via computer-generated citations and a search of key journals. Two online computer searches, Medline and SPORT database were conducted to locate published research on the effect of training on VO2max on children. A sample of the descriptive words used to locate relevant studies in research journals, conferences, and dissertation abstracts included: maximal oxygen uptake, aerobic capacity, aerobic fitness, cardiovascular fitness, children, puberty, growth and development and training. The majority of applicable studies came from the areas of pediatric exercise physiology (e.g., Medicine and Science in Sports and Exercise, Pediatric Exercise Science, International Journal of Sports Medicine, Journal of Pediatrics). Although ninety studies examining the effects of training on improving aerobic power in children were located, only 20 met the criteria for inclusion and contained the necessary descriptive statistics necessary to calculate the ESs.Coding Characteristics of the Studies
The studies in this review were coded according to methodological variables of interest known to influence VO2max in children. These characteristics included: the age and gender of the children, the intensity, frequency and duration of the exercise training, the presence or absence of a control group, the methodological design of the study [cross-sectional (XS) vs. pretest-posttest (PP) design], and the methods of testing for VO2max [bicycle ergometry (BE) vs. treadmill (TM)].The final criteria for inclusion were established as follows:
1. The purpose of the study was to determine the effects of training on VO2max in children.
2. The studies must have been conducted on a normal, healthy subjects (i.e., not asthmatics or obese)
3. Measurements of VO2max in ml·kg-1·min-1 must have been reported. It is important to note that although the typical VO2max criteria are not always met in children (i.e., a plateau during a progressive, incremental test was not achieved), other indices reported by the investigators to indicate the achievement as a maximal effort were considered. These indices included peak VO2, peak HR 10 b·min-1 from estimated maximal HR, and a respiratory exchange ratio > 1.1 since we did not want to eliminate studies that did not indicate a leveling of oxygen uptake (14).
4. Measurements of VO2max must have been taken utilizing a treadmill or a bicycle ergometer with open-circuit spirometry.
5. The appropriate descriptive statistics must have been included (i.e., means, standard deviations and n values. In some cases when the grand mean for the experimental or control groups were not provided, the necessary statistics were calculated from the individual data points provided by the individual investigators. Thus, every effort was made to include relevant studies whenever possible.
6. Studies must have included age groups of subjects that were 16 years or less (Table 1). The studies were then stratified by age groups to examine the impact of maturational differences.
7. The duration of the study must have been less than one year.ES Computation and Analyses
The ES was originally defined as the difference between the means of the experimental group (ME) and the control group (MC), divided by the control group standard deviation (SC). Thus the following formula can be applied for ES computation:ES = (ME - MC) / SC
This formula transforms the finding from an individual study into a common metric that can be submitted for further statistical analysis. That is, ESs can be averaged across studies to determine overall treatment effects, and they may be further stratified according to the coded characteristics. In many of the training studies, control subjects were not used. Rather, each subject served as his or her own control. Therefore, for the purposes of ES computation in this review, the pre-to-post-training changes in VO2max was used as the dependent measure to determine the overall effect of exercise whenever untrained control were not used. The pre-training VO2max was subtracted from the post-training VO2max to keep the algebraic sign of the ES positive. Thus, a positive ES indicates an improvement in VO2max at the completion of exercise training. The difference between the pre-and post-training measures for VO2max in studies that did not have a control group was divided by a pooled variance:
(post-training VO2max - pre-training VO2max) / pooled variance
According to Hedges (19), a pooled estimate of the variance provides a more precise estimate of the population variance. The pooled variance weighted for sample size was obtained by calculating the square root of the following formula:
Sp = [s12(n1 - 1) + s22 (n2 - 1)] / (n1 + n2 2)
for which Sp = the pooled standard deviation, s12, the variance for the experimental group or group one, s22 = variance for the experimental group or group two, n1 = the number of subjects in group one, and n2 = the number of subjects in group two.
Those studies, which utilized a control group, were subjected to the basic formula previously described for ES computation. In addition, all ESs were corrected for sample size bias (19). After stratifying the studies according to the coded characteristics of interest, the ESs from each of the categories were combined across studies and subsequently analyzed for significant differences. A students t-test was used to determine the significance of the effects of the study characteristics (training prescription, methodological design, test protocol, gender). Statistical significance was established at p<0.05 for the determination of significant differences among the coded variables.
RESULTS
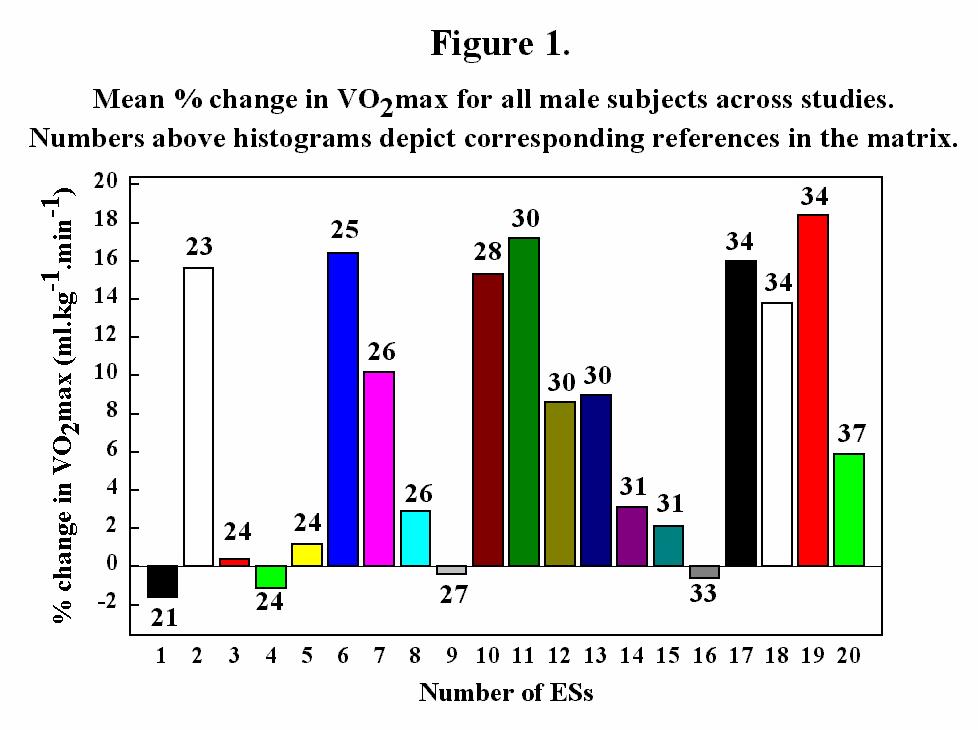
Ninety-one investigations were located that studied the effects of training on maximal aerobic power in children. Of those, 20 met the criteria for inclusion in this quantitative review and were subjected to further analyses. The 20 studies generated 32 ESs based upon a total of 562 subjects. Numerous studies were eliminated for inappropriately reporting of variables, or because the descriptive statistics essential for ES computation were absent. Other reasons for exclusion included a combination of age groups that made maturational influences impossible to discern from the effects of training, some investigations were not truly training studies, and some were in foreign languages that we could not arrange to have translated. Every attempt was made to consider those studies which met our inclusion criteria, including contacting individual authors for the necessary statistics to calculate the ESs. Table 1 summarizes the coded characteristics of the 20 studies and provides the accompanying ESs. Some investigations produced more that one ES because distinct groups (i.e., age differences or boys vs. girls) were reported separately. Figure 1- 3 depicts differences in mean percent change in VO2 (ml·kg-1·min-1) between pre and post tests for males, females and combined male and female groups.Figure 1- 3 depicts differences in mean percent change in VO2 (ml·kg-1·min-1) between pre and post tests for males, females and combined male and female groups.


The mean pre-VO2max for all of the subjects in this review was 47.2 ± 4.3, while the post-VO2max 50.1 ± 4.6. These data reflect the ability of children to demonstrate some improvement in maximal aerobic power after training. The analyses of the coded characteristics, however, demonstrated the impact of experimental design, subject differences (i.e., age and gender) and the training program on the outcomes of these studies.
An analysis of studies which utilized control groups (ES = 1.1 ± 0.1) versus those in which subjects served as their own controls (ES = 0.32 ± 0.2) revealed a significant difference in the outcome of maximal aerobic power (p<0.0009). Because only six ESs were generated from those studies that utilized a XS design (ES = 1.7 ± 0.3) as opposed to 24 ESs from the PP studies (ES = 0.63 ± 0.6), a meaningful analysis was impossible. Differences in subject characteristics indicated that children in the 11 to 13 year old range (15-25) (ES =1.1 ± 0.7) versus those in the 8 to 10 year old range (26-33) (ES = 0.47 ± 0.4) generated significantly higher VO2max data (p<0.02). Analyses of children less than 7 and greater than 13 were not possible because only 2 ESs were generated in each group. When studying the impact of gender, a majority of the studies utilized males as subjects. A total of 23 ESs were generated from male subjects, while only seven were from girls. The mean ES for both groups was 0.64 ± 0.6 and 1.0 ± 0.6, respectively, and revealed no difference. The testing protocol for determining VO2max revealed that neither the treadmill (ES = 0.75 ± 0.7) nor the cycle ergometer (ES = 0.94 ± 0.7) provided a discernable impact on the outcome of maximal aerobic power. Finally, the guidelines of the American College of Sports Medicine were used to determine sufficiency of the exercise prescription. The adequacy of the training protocol was measured against the standard frequency of three times per week, a minimum duration of 6 weeks, and sufficient exercise intensity. In many cases, the exercise intensity was difficult to determine because the individual investigators gave only limited details in their reports. Therefore, subjective decisions regarding exercise intensity were often necessary. The precise exercise prescription provided by the individual authors is included in Table 1. For those studies which reported an adequate training protocol, the mean ES was 1.2 ± 0.5, while the mean ES for those studies with an inadequate training protocol was 0.33 ± 0.2. These findings were statistically different (p<0.004). The results of these analyses are summarized in Table 2.
Table 2: Analyses of the Coded Characteristics.
SUBJECT CHARACTERISTICS: Age (years)
<7
>13
8-10
11-13Gender
Boys
GirlsN
2
2
11
17N
23
7MEAN ES ± SD
-0.4 ± 0.8
1.7 ± 0.3
0.5 ± 0.4
1.1 ± 0.7 p<0.02MEAN ES ± SD
0.6 ± 0.6
1.0 ± 0.6METHODOLOGICAL ISSUES:
Studies with controls
Studies without controlsPre-post designs
Cross-sectional designs
N
20
1124
6
MEAN ES ± SD
1.1 ± 0.1
0.3 ± 0.2 p<0.00090.6 ± 0.6
1.7 ± 0.3
TRAINING METHODS AND TESTING PROTOCOL:
Sufficient training stimulus
Insufficient training stimulusTreadmill testing
Cycle ergometer testing
N
15
1313
18
MEAN ES ± SD
1.2 ± 0.52
0.3 ± 0.2 p=0.0040.8 ± 0.7
0.9 ± 0.7
DISCUSSION
The purpose of this meta-analysis was to synthesize the research directed toward physical training in children and to provide a quantitative review of the specific impact of exercise on VO2max. The extent that children can improve aerobic power through training is unclear, particularly prior to puberty. It has been difficult to discern the effects of training for several reasons, including methodological pitfalls. Therefore, we attempted to elucidate the effects of research design on the magnitude of the ESs. In the first analysis, we determined that those studies which utilized untrained controls typically reported a significantly higher increase in VO2max after training, as opposed to those in which the subjects served as their own controls (p<0.0009). This finding supports the contention of Rowland and Boyajian (32) who recognized the need for matched controls when studying children, as well as the desirability of PP rather than XS designs. An analysis of the descriptive statistics indicate that XS designs clearly generated higher ESs as opposed to those studies that were PP (ES =1.7 vs. 0.63). These two findings demonstrate the need to address methodological weaknesses in order to minimize or eliminate the effects of confounding variables such as growth and maturation particularly inherent in XS designs. The potential impact of a weak design, particularly in studies of prepubescent children, seriously impedes the investigators ability to attribute the increases in VO2max to the training protocol.An analysis of the subjects' age revealed that children who were in the 11 to 13 year old range improved their aerobic power by more than a standard deviation (ES =1.1), while those in the 8 to 10 year old range improved by approximately one-half standard deviation after training (ES = 0.47). This significant finding (p<0.02) supports the research which states that training is much less effective during the first decade of life. The physiologic support for this finding rests upon the observation that a lack of hormonal control exists in young children (6). It is impossible to state that all of the children in the younger age group (8 to 10 years) were indeed prepubescent or that those in the older group (11 to 13 years) were pubescent; nevertheless, the magnitude of the difference in the mean ESs indicates there is very likely a substantive improvement in VO2max as a function of age. In their study of the development of aerobic power in young athletes, Baxter-Jones et al (33) reported that when age, height, and weight were controlled for, VO2max increased significantly with pubertal status. In other words, VO2max increases proportionately to body mass in both sexes. Our data support these findings because the differences in the overall training effect manifested in VO2max were significantly higher in the older group.
Any significant differences between males and females in our study was impossible to determine, in large part due to the paucity of studies in which females were used as subjects. Although only seven ESs were from an analysis of the effects of training in girls, the mean ES was 1.0. In contrast, twenty-three ESs were computed from the studies of boys, resulting in a mean ES of 0.64. These data indicate that both boys and girls demonstrate improvement in aerobic power after training; however, it is clear that additional research should be directed toward the impact of training in young girls to define clearly the effects of pubertal status. While it is known that girls are far less physically active than boys prior to puberty for varying reasons, such as social influences, it would be interesting to study the spectrum of physiologic responses that could account for the differences in VO2max before and after puberty with training. Although the mean ES suggests that girls could be more trainable than boys, we can not discount the possibility of low initial fitness levels as an explanation. It is clear that differential adaptation to training in boys and girls requires additional investigation.
To assess the effect of training sufficiency on maximal aerobic power, a separate analysis on the quality of the exercise prescription was conducted. Those studies that maintained an exercise protocol which consisted of a minimum training frequency of three times a week, a duration of 6 weeks and an intensity that was equivalent to or greater than 70% of the maximum HR were considered to be sufficient. All other exercise-training prescriptions were considered insufficient. The mean ES for those studies which utilized a sufficient training stimulus was 1.2 ± 0.5 and 0.33 ± 0.2 for those studies with an insufficient stimulus (p<0.004). This analysis indicated that the training stimulus, particularly exercise intensity, had a highly significant impact on the improvements in VO2max in children perhaps to the same degree as in adults. We are somewhat cautious about the interpretation of this finding because of the inadequate documentation of training intensity in all of the studies included in this review. Consequently, it is difficult to state with certainty the ability of the training protocol to cause favorable alterations in VO2max. These ES data are corroborated by the results of one of the few well-controlled,longitudinal studies of the effects of training on children. Rowland and Boyajian (32) studied 24 children (ages 10 to 13) who participated in an aerobic training program with an exercise prescription that met our criteria for a sufficient training stimulus (mean activity HR of 166 b·min-1). After 12 weeks of training, the children improved their VO2max by 6.5% (p <0.05). The authors concluded that training can improve VO2max in children, however, their ability to manifest large improvements is somewhat limited in comparison to their adult counterparts. They hypothesized that several contributing factors may blunt training responses in prepubescent children, including higher initial levels of fitness and physical activity. In our review, the pre VO2max for all of the children was 47.1 ± 4.3, which is considered to be relatively high for the age groups we studied. The post VO2max was 50.1 ± 0.5 which reflects a 6.0 % increase. Therefore, there is sufficient evidence to suggest that training can increase maximal aerobic power in children, but the magnitude of the increase is probably lower than what can be reasonably expected in adults.
The last analysis we conducted was a study of the test protocol used by the individual investigators to test VO2max before and after training. It was a necessary prerequisite that all tests were conducted with open circuit spirometry. Since it is well documented that a TM test generates a VO2max that is on the average 10 to 15% greater than those conducted on a cycle ergometer due to the significant increase in the amount of muscle mass involved, we sought to determine if these differences would be reflected in the children's' maximal aerobic power. Interestingly, the mean ES for the tests conducted on the TM was 0.75 ± 0.7 while the mean ES for the tests on the BE was 0.94 ± 0.7. We speculated that the familiarity with the motion of bicycling in most children may actually cause the BE to be a preferential mode of testing for maximal aerobic power. The TM, on the other hand, requires somewhat of a learning effect before a subject is comfortable. The lack of familiarity with the TM may be especially relevant in children. Additional study is needed to determine if bicycle familiarity overrides the impact of a using a greater body mass during TM testing, particularly in very young children.
CONLCUSION
Our quantitative review clearly supports the position that children are indeed trainable, but that the magnitude of the training response may be somewhat lower than their adult counterparts. It appears that pubertal status plays the most significant role in determining the effects of training on VO2max, but there is insufficient evidence to determine the effects of the training stimulus, particularly due to the lack of properly documented exercise intensities in past research. Furthermore, longitudinal data are clearly preferential, particularly in studies examining the effects of training as a function of pubertal status. The critical stage of maturity where training may exert its greatest impact remains speculative; thus, there is a need for additional inquiry to elucidate this perplexing question. The answer is difficult to discern in large part due to the inability to invasively study the adaptive mechanisms of training such as myocardial contractility, plasma volume, sympathetic nervous activity, peripheral oxygen extraction, and concentrations of aerobic enzymes such as succinate dehydrogenase (39). How changes in these key variables are associated with pubertal status is unclear.Finally, as a result of this integrative review, we provide the following recommendations for future research which may augment our current understanding of training adaptations in children:
(1) Design studies that control for maturation and growth to clearly delineate the effects of training as a function of pubertal status.
(2) Conduct research that will demonstrate any potential gender differences in children of all ages.
(3) Seek the utilization of noninvasive methods which will elucidate the adaptive mechanisms involved in improving VO2max.(4) Determine the impact of the training stimulus (particularly exercise intensity) and the most effective modes of training that could induce favorable adaptations. In the research included in this review, most investigators trained children by running. Only a few used cycling and interval training, and fewer still utilized swimming. There was not enough variability in the mode of training to conduct a meaningful analysis.
(5) Evaluate the typical bursts of sustainable activity in children. Perhaps these data would either support or refute the notion that children are less trainable because they are unable to adhere to a consistent rigorous program of exercise training.It is likely that the results of such inquiry will provide answers that would positively impact the conditioning status of both healthy and physically limited children (e.g., asthmatics), and will provide both clinicians and researchers with reasonable expectations for physiologic responses to exercise in young children through their adolescent years.
ACKNOWLEDGMENT: The research for this project was supported, in part, by a Research and Disciplinary Grant from Bloomsburg University, Pennsylvania.
REFERENCES
1. Godfrey, S. Exercise testing in children. London: W. B. Saunders, 1974.
2. Katasura, T. Influence of age and sex on cardiac output during submaximal exercise. Ann Physiol Anthropo 1986;5:39-57.
3. Rowland, T.W., Staab, J., Unnithan, V., and Siconolfi, S. Maximal cardiac responses in prepubertal and adult males. Med Sci Sports Exerc 1988, 20(Suppl.), S32.
4. Mirwald, R., Bailey, D. Cameron, N. & Rasmussen, R. Longitudinal comparison of aerobic power in active and inactive boys aged 7 to 17 years. Ann Hum Biol 1981;8:405-414.
5. Kobayashi, K., Kitokazu, K., Miura, M. & Sodeyama, H. Aerobic power as related to growth and training in Japanese boys: a longitudinal study. J Appl Physiol 1978;44:666-672.
6. Katch, V.L. Physical conditioning of children. J Adol Health Care 1983;3:241-246.
7. Borms, J. The child and exercise: An overview. J Sports Sci 1986;4:3-20.
8. Bar-Or, O. Trainability of the prepubescent child. Physician Sports Med 1989;17:65-81.
9. Eisenman, P.A. & Golding, L.A. Comparison of effects of training on VO2 max in girls and young women. Med Sci Sports and Exerc 1975;7:136-138.
10. Mayers, N. & Gutin, B. Physiological characteristics of elite prepubertal cross-country runners. Med Sci in Sports and Exerc 1979;11:172-176.
11. Rowland, T.W. Aerobic responses to endurance training in prepubescent children:A critical analysis. Med Sci in Sports and Exerc 1985;17:493-497.
12. Vaccaro, P. & Mahon, A. Cardiorespiratory responses to endurance training in children. Sports Med 1987;4:352-363.
13. Pate, R. & Ward, D. Endurance exercise trainability in children and youth. In B.J. Sharkey (Ed.), Advances in Sports Med Fit (Vol. 3., 37-55). Chicago: Yearbook Medical.
14. Sady, S. Cardiorespiratory exercise training in sports medicine. Clin Sports Med 1986;5:493-514.
15. Krahenbuhl, G.S., Skinner, J.S., and Kohrt, W.M. Developmental aspects of maximal aerobic power in children. Exercise and Sports sciences reviews 1985, 13; 503-538.
16. Cunningham, D.A., Paterson, D.H., and Blimkie, C.J.R. The development of the cardiorespiratory system with growth and physical activity. In R.A. Boileau (Ed.), Advances in Pediatric Sport Sciences. 1984, pp. 85-116. Human Kinetics, Champaign, IL.
17. Shephard, R.J. Physical activity and growth. Year Book Medical Publishers, Chicago, IL, 1982.
18. Glass, G.V. Integrating findings: The meta-analysis of research. Rev Research Edu 1977;5:351-379.
19. Hedges, L.V. & Olkin, I. Statistical Methods for Meta-Analysis 1985. NewYork: Academic Press.
20. Bar-Or, O. & Zwiren, L. Physiological effects of increased frequency of physical education classes and of endurance conditioning on 9 to 10 year old girls and boys. In O. Bar-Or (Ed.), Pediatric Work Physiology: Proceedings of the Fourth International Symposium. 1973:114-126.
21. Benedict, G., Vaccaro, P. & Hatfield, B. ght week precision jump rope program in children. Am Correc Ther 1985;5:108-111.
22. Brown, C., Harrowere, J. & Deeter, M. The effects of cross-country running on pre-adolescent girls. Med Science Sports Exerc 1972;4:1-5.
23. Conn, C.A., Schemmel, R. Smith, B. Ryder, E. Heusner, W. & Ku, P. Plasma and erythrocyte magnesium concentrations and correlations with maximum oxygen in nine to twelve year old competitive swimmers. Magnesium 1988;7:27-36.
24. Cumming, G. Goulding, D. & Baggley, G. Failure of school physical education to improve cardiorespiratory fitness. Can Med Assoc J 1969;101:69-73.
25. Docherty, D. Wenger, H. & Collis, M. The effects of resistance training on aerobic and anaerobic power of young boys. Med Sci Sports Exerc 1987;19;389-392.
26. Ekblom, B. Effect of physical training in adolescent boys. J Appl Physiol 1969;27:350-355.
27. Gilliam, T. & Freedson, P. Effects of a twelve-week school physical fitness program on peak VO2, body composition, and blood lipids in 7 to 9 year old children. Int J of Sports Med 1980;1:73-78.
28. Koch, G. & Eriksson, B.O. Effect of physical training on pulmonary ventilation and gas exchange during submaximal and maximal work in boys aged 11-13 years. Scan J Clin Lab Invest 1973;31:87-94.
29. Lustier, L. & Buskirk, E. Effects of an endurance training regimen on assessment of work capacity of prepubertal children. Annals of the New York Academy of Science. 1977;30:734-747.
30. Massicotte, D. & MacNab, R. Cardiorespiratory adaptations to training at specified intensities in children. Med Sci Sports Exerc 1974;6:242-246.
31. Mocellin, R. & Wasmun, U. Investigation of the influence of a running training programme on the cardiovascular and motor performance capacity of 53 boys and girls of a second and third primary class. In O. Bar-Or (Ed.), Pediatric Work Physiology:Proceedings of the Fourth International Symposium. 1973, 279-288.
32. Rowland, T.W. & Boyajian, A. Aerobic response to endurance exercise training in children. Pediatrics 1995;96:654-658.
33. Stewart, K. & Gutin, B. Effects of training on cardiorespiratory fitness in children. Res Quart 1976;47:110-120.
34. Sunberg, S. & Elovainio, R. Cardiorespiratory function in competitive endurance runners aged 12-16 years compared with ordinary boys. Acta Paediatrica Scan 1982;71:987-992.
35. Vaccaro, P.& Clarke, D.H. Cardiorespiratory alterations in 9 to 11 year old children following a season of competitive swimming. Med Sci Sports 1978;10;204-207.
36. Yoshida, T.,Ishiko, I. & Muraoka, I. Effects of endurance training on cardiorespiratory function of 5 year old boys. Int J Sports Med 1980;1:91-94.
37. Yoshizawa, S.A., Honda, H. Urushibara, M. & Nakamura, N. Effects of endurance run on the cardiorespiratory system in young children. J Hum Ergology 1990;19:41-52.
38. Baxter-Jones, A., Goldstein, H., & Helms, P. The development of aerobic power in young athletes. J Appl Physiol 1993;75:1160-1167.
39. Holloszy, J.O. Biochemical adaptations to exercise: aerobic metabolism. Exerc Sport Sci Rev 1973;1:45-71.
Address all correspondence to: Serge P. von Duvillard, PhD, Director-Human Performance Laboratory, Department of Physical Education & Exercise Science, University of North Dakota, PO Box 9037 Grand Forks, ND 58202, (701) 777-4345 (office), (701) 777-3531 (Fax)E-mail: vonduvil@badlands.nodak.edu
Copyright ©1999
American Society of Exercise Physiologists
All Rights Reserved