AMERICAN SOCIETY
OF EXERCISE PHYSIOLOGISTS
Founded, 1997
Journal
of Exercise Physiologyonline
ISSN
1097-9751
An International Electronic
Journal for Exercise
Physiologists
Volume 2 Number 4 October
1999
Systems Physiology:
Cardio-pulmonary
R.W. GOTSHALL1, J. GOOTMAN1, W.C. BYRNES2, S.J. FLECK3 and T.C. VALOVICH2
1Colorado State University, Exercise and Sport Science, Fort Collins, CO; 2University of Colorado, Kinesiology, Boulder CO; and 3Colorado College, Sport Science, Colorado Springs, CO
R.W. GOTSHALL, J. GOOTMAN, W.C. BYRNES, S.J. FLECK and T.C. VALOVICH. Noninvasive characterization of the blood pressure response to the double-leg press exercise. JEPonlineVol 2 No 4, 1999. The purpose of the study was to measure arterial blood pressure with the Finaprestm noninvasive, continuous blood pressure monitor (FBPM) to characterize the continuous blood pressure response during three sets of a 10-repetition maximum double-leg press exercise. Seven recreational weight lifters volunteered for this study. Preliminary sessions determined the 10-repetition maximum (10-RM) for the double-leg press. Subjects lifted to a metronome cadence and were coached to avoid the Valsalva maneuver. During the experimental session, subjects were instrumented for blood pressure measurements by the FBPM. The FBPM used a cuff placed on the middle finger of the right hand, which was maintained at heart level. Subjects completed three sets of 10-RM lifts. Similar to previously reported studies using blood pressure via intra-arterial canulation: within a single repetition, peak pressure was developed as the legs initiated the concentric lift from the flexed position; lowest pressures were developed as the legs became fully extended, and the blood pressure increased with each successive repetition within a set. Additionally, blood pressure increased significantly with each subsequent set (peak systolic blood pressures: set 1- 238±18; set 2 - 268±18; set 3 - 293±21 mmHg). In conclusion, blood pressure responses to the leg press exercise increase with each repetition and also with each successive set, at least for three sets. Therefore, the highest pressures during the leg press were achieved as the lift was initiated from the flexed position, with further increases as repetition and set numbers increased.
Keywords: weight lifting, cardiovascular, Finaprestm
INTRODUCTION
The blood pressure increase above resting values during weight lifting is variable and can be of considerable magnitude (1-4). Direct intra-arterial recordings of blood pressure (3-6) have shown that blood pressure changes variably during the concentric and eccentric phase of a weight lifting exercise, and that the magnitude of the blood pressure response increases with each successive repetition. Peak systolic pressures in excess of 300 mmHg have been recorded by this method during the double-leg press exercise (2,6), especially when a Valsalva maneuver is performed during the lift. Because of the dynamic nature of the blood pressure response to weight lifting, intermittent blood pressure determinations by standard arm cuff and auscultation are not representative of either the magnitude of the blood pressure change nor of the characteristic response to the resistance exercise (7). While direct intra-arterial blood pressure determinations can fully characterize the blood pressure response to resistance exercise, there is significant risk associated with this invasive technique such as pain, arterial spasm, blood clots, bleeding, and vaso-vagal syncope.
Due to the limitations of the above two methods of determining blood pressure, a non-invasive, continuous blood pressure monitor would be of value. The Finaprestm Blood Pressure Monitor (FBPM) offers the capability of noninvasive, continuous blood pressure monitoring, similar to intra-arterial recording. The FBPM is based on the method reported by Penaz in 1973 (8) and is a photoplethysmographic technique applied noninvasively to the finger. Blood pressure is recorded beat-to-beat with an arterial pressure waveform that is typically indistinguishable from that recorded with an intra-arterial catheter (8-11). The FBPM has been compared with both intra-arterial recordings of blood pressure and standard arm cuff blood pressures at rest and during exercise, with variability of agreement (12-15). However, it has been suggested that FBPM blood pressures would be more accurate if calibrated to brachial blood pressure (16).
The purpose of this study was to use the FBPM to noninvasively characterize the blood pressure waveform response during three sets of a 10-repetition maximum double-leg press exercise. It was hypothesized that systolic blood pressure would increase during eccentric contractions and decrease with concentric contractions, and would increase with each successive repetition within a set of 10 repetitions, and with each successive set of three sets.
METHODS
Seven healthy, nonsmoking males between the ages of 20 and 35 years volunteered as subjects for this study. Subjects had no current or past competitive experience with resistance training. They were familiar with weight lifting and had recreational experience as determined by questionnaire. The study was explained to each subject and informed consent obtained. The study had Colorado State University Institutional Review Board approval for human subject research.
Subjects were instructed to abstain from any strenuous physical activity for 48 hours prior to their testing sessions. In addition, subjects were instructed to abstain from alcohol or caffeine for 24 hours prior to all testing sessions. Preliminary testing sessions were held for the purpose of obtaining the subject's true ten-repetition maximum (10-RM) for the double-leg press exercise and familiarizing them with the protocol. Determination of the 10-RM was accomplished on the same equipment and in the same position as for the experimental lifts. The repetitions were performed to a metronome-based cadence of 3 seconds for the concentric phase of the lift and 3 seconds for the eccentric phase of the lift. Subjects were coached to avoid a Valsalva, although this was difficult to avoid in the final repetitions of a set. During the preliminary sessions, if the subject was able to complete 10 repetitions at a given weight, a greater weight was selected and the subject again was asked to give maximal effort to complete ten repetitions in the next preliminary testing session 2 days later. By the third such session, the true 10-RM for the individual was determined. The greatest weight with which a subject was able to complete ten repetitions was recorded as the 10-RM. Those subjects whose 10-RM was determined prior to the third preliminary session still completed the second and/or third session in order to confirm their 10-RM weight. Subjects then reported the following week to the laboratory for the experimental session. The experimental session consisted of a lifting protocol consisting of a 10-repetition double-leg press at the predetermined 10-RM for three sets. A three-minute rest period was allowed between sets. The 10-RM protocol was chosen to elicit large changes in blood pressure.
For blood pressure monitoring, subjects were instrumented with the Finaprestm Blood Pressure Monitor (Model 2300, Ohmeda, Madison, WI) finger cuff, sized to the middle phalanx of the middle finger of the right hand. A wood splint was taped to the subjects middle finger to prevent bending of the finger to ensure uninterrupted blood flow to the finger cuff during the straining associated with the lift. The right arm was then placed in a sling to keep the finger at heart level throughout the protocol. The Finaprestm blood pressures were continuously recorded on a strip chart recorder (Gould 2400, Gould Instruments, Cleveland, OH). Subjects first sat quietly for 10 minutes positioned in the leg press machine to collect baseline data of all cardiovascular measures obtained. Both standard auscultation and Finaprestm blood pressures were determined. Subsequently, the 3 sets of 10 repetitions of leg press were performed. Finaprestm blood pressures were recorded prior to and throughout each set.
FBPM blood pressure during the lift was characterized by the peak and nadir of pressures achieved with each repetition as shown in figure 1. Repeated-measures ANOVA was then applied to the data for the 10 repetitions within each set, and across the average of the final 2 repetitions among the three sets. Fishers LSD post-hoc test was applied if a significant f-ratio was determined by the ANOVA. Significance was accepted at p<0.05.
RESULTS
Table 1 shows the Finaprestm blood pressure values at rest before the initial series of lifts.
Table 1: Finaprestm Blood Pressure Values (mmHg) at Rest
| SBP | DBP | Mean BP | |
| FBPM | 121±13 | 75±13 | 90.2±13 |
Figure 1 is a representative recording of the blood pressure response to the double-leg press. For clarity, only 1 complete repetition is shown. Pressures varied within each repetition achieving both a peak and a nadir. The peak pressure occurred with the initiation of the concentric phase of the lift from the legs-flexed (90-degree knee angle) position, with decreasing pressures occurring during the concentric phase until the legs were at the maximum leg extension. The blood pressure subsequently increased as the weight was lowered during the eccentric phase until the knees reached the 90-degree position again.

Figure 1: Sample of blood pressure recording during one complete leg press repetition. C, concentric phase; E, eccentric phase; arrow designates point in cycle where legs were maximally extended.
Table 2 shows the mean values for the SBP and the mean blood pressures at rest preceding each set, and again at the final repetition of each set when the highest values were obtained. SBP increased significantly from rest to peak exercise for each set. Resting SBP values increased by the period preceding the final set. Exercise peak SBP values increased progressively from each set to the next, being the highest by the end of the final set. The same pattern of changes was observed for the mean blood pressures. These patterns are shown graphically in Figures 2 and 3.
Table 2: Blood Pressure (mmHg) for Each Set of Double-Leg Press
| Set 1 | Set 2 | Set 3 | |
| SBP | |||
| Rest | 121±13a | 128±18a | 142±18b |
| Exercise | 238±18*,a | 268±18*,b | 293±21*,c |
| Mean BP | |||
| Rest | 90.2±13a | 97±18a | 105±18b |
| Exercise | 173±18*,a | 182±16*,b | 212±18*,c |
Values are means ± SD. Letters (a,b,c) designate significance within rows for each variable at p<0.05, letters different from one another are significantly different. The asterisk (*) designates significance between the resting value and the exercise value for each variable for each set.

Figure 2: The pattern of systolic and diastolic
blood pressure response to 3 sets of 10-RM double-leg press lifts.
Lowest value preceding each set is the resting blood pressure.
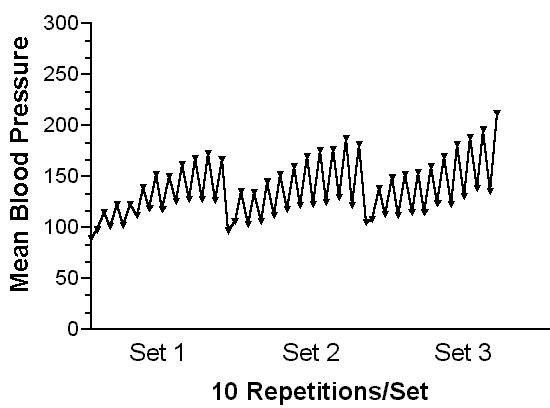
Figure 3: The pattern of mean blood pressure
response to the 3 sets of 10-RM lifts.
DISCUSSION
The principal findings of this study were that systolic and mean pressures increased progressively within each set with the number of the repetition, and also increased with each subsequent set of double-leg presses, a novel observation. Also, of interest is the finding that within each repetition, blood pressures varied markedly. The highest pressure within a single repetition occurred as the concentric phase was initiated, and the lowest pressure was obtained when the legs reached the end of the concentric phase, with the legs maximally extended. Thus, blood pressures declined during the concentric phase and increased during the eccentric phase.
Studies (2, 6,9) that have characterized the continuous blood pressure response to weight lifting through the use of intra-arterial canulation and blood pressure recordings have shown the same specific blood pressure patterns as demonstrated with the FBPM in the present study (5,6). Recordings from intra-arterial cannulation during the double-leg press performed to failure (2,6) look remarkably similar to those shown in figure 1of the current study obtained with the FBPM. In two separate studies, MacDougall and colleagues (2,6) recorded blood pressures intra-arterially during the double-leg press. Peak pressures occurred at the initiation of the concentric phase with the legs at 90 degrees and the nadir occurred as the legs reached extension (2,6). This was confirmed by measuring the joint angles throughout the lift (6). This pattern was identical to the current study. The potential mechanisms responsible for this pattern include the possibility that at the beginning of the lifting phase, with the knee joint angle at 90 degrees, the leg extensors are at their weakest point on the strength curve. This would require a greater effort relative to maximum effort and generate a greater blood pressure response (17). As the legs are extended, they approach the strongest position as extension is achieved, reducing effort and decreasing blood pressure. Upon lowering the weight through the eccentric phase, the relative effort is increased over time, approaching the weakest point on the strength curve, and eliciting the highest blood pressure response (17).
In these same previous studies using intra-arterial recordings of blood pressure, the peak blood pressures increased with each successive repetition until failure (2, 6). Again, an identical pattern of response as measured in the current study. The peak pressures obtained in the studies by MacDougall et al. (2,6) were generally higher than those reported in the present study, however, the subjects in the previous studies performed Valsalva maneuvers while lifting, while performance of the Valsalva was discouraged in the current study. Performance of the Valsalva during the lift contributes to the elevation of blood pressures during lifting (2,4,6,18). McDougle, McCartney and colleagues (6,17) have hypothesized that this progressive increase in blood pressure throughout a set is related to the rising effort with each successive repetition. As the muscle approaches fatigue, more relative effort is required, accessory muscles may be recruited, a full or partial Valsalva may be performed, and muscle nociceptors may be stimulated. Any and all of these may occur and contribute to elevating the blood pressure.
To our knowledge, the present study is the first report demonstrating that the peak blood pressures during lifting increased with subsequent sets. That is, the peak blood pressure of set 3 was greater than that in set 1. Although the resting blood pressure value preceding each set also increased by set 3, the change with the lifting from these resting values was also increased with each subsequent set. Thus, this progressive elevation in lift-generated pressures is not entirely explained by the increased resting values. The potential reasons for this progressive increase in blood pressure with subsequent sets of leg lifts may mirror those described above for the similar pattern observed within each set (6, 17). However, this effect requires further investigation.
There are technique-specific limitations that apply to the FBPM. First, the finger cuff must be properly sized to the individual. The cuff is marked similar to arm cuffs for proper sizing. Secondly, the cuff must be placed snuggly without being either too loose or too tight. The instrument will detect most conditions in which the cuff is too loose or too tight. However, to ensure proper fit, brachial cuff blood pressures were routinely taken to determine if the FBPM and the cuff values were in close agreement. If not, the cuff was re-tensioned until the FBPM and cuff values agreed within 5%. Finally, there is at least one report that blood pressure values with the FBPM will drift over time if the cuff is not deflated and the hand muscles exercised (19). In the current study the time period of measurements was short, so there was no baseline drift. If longer protocols are used (greater than 30 minutes), then periodic cuff removal with hand exercise is required. Replacing the cuff and re-establishing agreement with manual brachial cuff pressures should permit long term monitoring. Other possible influences on the values recorded by the FBPM are failure to keep the hand at heart level, motion artifacts, and muscle tension in the hand that can compress the artery. All of these were obviated in the present study by placing the hand in a sling at heart level to maintain position and reduce movement. Additionally, the finger with the cuff was splinted to prevent bending the finger with exertion during the lift.
In conclusion, this study has provided non-invasive
characterization of the blood pressure response to the double-leg press.
The characteristics of the blood pressure response to the double-leg press
clearly indicated the dynamic changes that occur during weight lifting.
The data confirm those shown with intra-arterial recordings of blood pressure
in that the peak pressures obtained increase with each successive lift,
and add the observation that the peak pressures increase with each subsequent
set, at least up to three sets. The potential effect of these high
pressures on the heart is indicated by the change in rate-pressure product
[heart rate times SBP] from resting values of 14.5 x 103
to 43.4 x 103 at peak blood pressures.
These data provide information that is relevant to understanding the cardiovascular
response to weight lifting, and to the eventual determination of the safety
of weight lifting for special populations (e.g. hypertensives, older adults,
cardiac patients).
REFERENCES
1. Hill DW, Butler
SD. Hemodynamic responses to weightlifting exercise. Sports Med 1991;12:1-7.
2. MacDougall JD,
Tuxen D, Sale DG, Moroz JR. Arterial blood pressure response to heavy exercise.
J
Appl Physiol 1985;58:785-90.
3. McCartney N,
McKelvie RS, Martin J, Sale DG, MacDougall JD. Weight-training-induced
attenuation of the circulatory response of older males to weight lifting.
J
Appl Physiol 1993;74:1056-60.
4. Narloch JA, Brandstater
ME. Influence of breathing technique on arterial blood pressure during
heavy weight lifting. Arch Phys Med Rehabil 1995;76:457-62.
5. Fleck SJ, Dean
LS. Resistance-trainjng experience and the pressor response during resistance
exercise. J Appl Physiol 1987;63:116-20.
6. MacDougall JD,
McKelvie RS, Moroz DE, Sale DG, McCartney N, Buick F. Factors affecting
blood pressure during heavy weight lifting and static contractions. J
Appl Physiol 1992;73:1590-7.
7. Wiecek EM, McCartney
N, McKelvie RS. Comparison of direct and indirect measures of systemic
arterial pressure during weightlifting in coronary artery disease. Amer
J Cardiol 1990;66:1065-9.
8. Penaz J. Photoelectric
measurement of blood pressure, volume and flow in the finger. In: Albert
R, Vogt WS, Helberg W, eds. Digest of the International Conference on Medicine
and Biological Engineering. Dresden: Conference Committee of the Xth International
Conference on Medicine and Biological Engineering; 1973:104
9. Imholz BPM, Settles
JJ, Van Der Meiracker AH, Wesseling KL, Wieling W. Non-invasive continuous
finger blood pressure measurement during orthostatic stress compared to
intra-arterial pressure. Cardiovasc Res 1990;24:214-21.
10. Imholz BPM, Van Montfans
GA, Settles JJ, Van Der Hoven GMA, Karemaker JM, Wieling W. Continuous
noninvasive blood pressure monitoring: reliability of Finapres device during
Valsalva manoever. Cardiovasc Res 1988;22:390-7.
11. Parati G, Casadei
R, Gropelli A, DiRienzo M, Mancia G. Comparison of finger and intra-arterial
blood pressure at rest and during laboratory testing. Hyperten
1989;13:647-55.
12. Imholz BPM, Wieling
W, Van Montfans GA, Wesseling KH. Fifteen years experience with finger
arterial pressure monitoring: assessment of the technology. Cardiovasc
Res 1998;38:605-16.
13. Blum V, Carriere
EGJ, Kolsters W, Mostered WJ, Schiereck P, Wesseling KH. Aortic and peripheral
blood pressures during isometric and dynamic exercise. Int J Sports
Med 1997;18:30-4.
14. Hildebrandt W, Schutze
H, Stegemann J. On the reliability of the Penaz cuff during systemic and
local fingertip vasodilation at rest and in exercise. Europ J Appl
Occupat Physiol 1991;62:175-9.
15. Silke B, Spiers JP,
Boyd S, Graham E, McParland G, Scott ME. Evaluation of non-invasive blood
pressure measurement by the Finapres method at rest and during dynamic
exercise in subjects with cardiovascualr insufficiency. Clin Autonom
Res 1994;4:49-56.
16. Silke B, McAuley
D. Accuracy and precision of blood pressure determination with the Finapres:
an overview using re-sampling statistics. J Human Hyperten 1998;12:403-9.
17. McCartney N. Acute
responses to resistance training and safety. Med Sci Sports Exerc
1999;31:31-7.
18. Linsenbardt
ST, Thomas TR, Madsen RW. Effect of breathing techniques on blood pressure
response to resistance exercise. Br J Sports Med 1992;26:97-100.
19. Ristuccia HL, Grossman
P, Watkins LL, Lowan B. Incremental bias in Finapres estimation of baseline
blood pressure levels over time. Hyperten 1997;29:1039-43.
Correspondence: Robert
Gotshall, Ph.D., Colorado State University, Exercise and Sport Science,
Fort Collins, CO 80523-1582 Voice: (970) 491-6374, Fax:
(970) 491-0445, email: gotshall@cahs.colostate.edu
Copyright ©1999
American
Society of Exercise Physiologists. All Rights Reserved.
ASEP Table of Contents
JEPonline October 1999 issue
JEPonlineGuidelines
