Auscultation:
Listening to Determine Dysfunction
Mark Kaelin, MS,CSCS
Exercise Physiologist
Pulmonary Rehabilitation
Program Coordinator
Southern Indiana Rehabilitation
Hospital
New Albany, IN
See also: Physical
Assessment: An Often Over-Looked Portion of Exercise Testing and Prescription
Auscultation is the process
of listening for sounds produced in the body to identify normal or abnormal
sounds and to aid in diagnosis. Exercise Physiologists cannot diagnose
conditions. Auscultation is a assessment tool to determine the limiting
factors to exercise. This article is limited to those sounds generated
in the lungs. However, before we can cover how to ausculate, a brief review
of the respiratory system and the thorax is needed.
Anatomy of the Respiratory
System and Thorax
The respiratory system can
be separated into two tracts (upper and lower) The upper respiratory tract
is comprised of the nose, paranasal sinuses, pharynx, and the larynx.
The purpose of this tract is to purify, warm, and humidify ambient air
before it reaches the gas exchange units. The lower respiratory tract begins
with the trachea, the right main bronchus which divides into three lobar
or divisions of the lung (upper, middle, and lower), the left main bronchus
which divides into two lobes (upper and lower), followed by the bronchioles,
and terminating at the alveoli (air sacs). In this tract, there are approximately
23 generations of airways; the first 16 are conducting airways while the
last seven are respiratory airways ending in approximately 300 million
alveoli, which form the gas exchange surface (1).
Figure 1. Anatomy
of the Respiratory System

The bony thorax is an
osseo-cartliginous cage containing and protecting the organs of respiration
and circulation. Its skeletal framework is comprised of the sternum, coastal
cartilage, ribs, and 12 thoracic vertebrae. Auscultation of the lungs involves
the thorax and the lower respiratory tract, its imperative that exercise
physiologists are familiar with anatomy and anatomical landmarks so one
knows where and what they are listening to. The trachea is located at the
base of the neck and extends 10-12 cm ( 3.7 - 4.5 inch) to the main carina;
a keel shaped ridge at the lower end of the trachea separating the openings
of the left and right bronchus (2, 4-6).
The bronchi can be auscultated at the upper manubrium.
Figure 2. Anterior
View of the Thorax

Listening to the Lungs
The lungs are auscultated
with the diaphragm on the chest piece of a stethoscope with the patient
breathing slowly and deeply thorugh their mouth. The anatomical sites for
lung auscultation are illustrated in below.
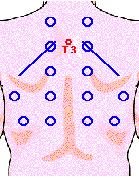
Figures 3 and 4.
Sites for Auscultation of the Lungs
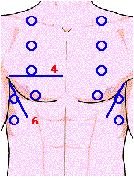
There are some common errors
to avoid:
1. Listening to
breath sounds through a patients gown or clothes.
2. Allowing tubing to rub
against bed rails or patients clothes.
3. Interpreting chest hair
sounds as adventitious* sounds.
4. Auscultating on the convenient
places only (3, 7).
*Adventitious sounds: added
sounds, or those superimposed on a patient's
underlying breath sounds that usually indicate disease.
Normal breath sounds consist
of those heard over the entire lung field and consist of an inspiratory
and expiratory phase. They are classified as:
Tracheal: These breath
sounds are high-pitched and loud, with a harsh and hollow (or "tubular)
quality. The inspiratory and expiratory phases are of equal duration, and
there is a definite pause between phases. Tracheal breath sounds usually
have very little clinical usefulness.
Bronchial: Normally
heard over the upper manubrium, these breath sounds directly reflect turbulent
airflow in the main-stem bronchi. They are loud and high-pitched but not
quite as harsh and hollow as tracheal breath sounds, the expiratory phase
is generally longer than the inspiratory phase, and there is usually a
pause between the phases.
Bronchovesicular:
These breath sounds are normally heard in the anterior first and second
intercostal spaces and posteriorly between the scapulas, where the main-stem
bronchi lie. The inspiratory and expiratory phases are about equal in duration,
with no pause between phases. Bronchovesicular sounds are soft and less
harsh than bronchial breath sounds and have a higher pitch than vesicular
sounds.
Vesicular: Audible
over peripheral lung fields, these breath sounds are soft and low-pitched,
without the harsh, tubular quality of bronchial and tracheal breath sounds.
The inspiratory phase is about three times longer than the expiratory,
with no pause between phases (7).
Breath sounds are considered
abnormal if they are heard outside their usual location in the chest or
if they are qualitatively different from normal breath sounds (e.g. decreased
or absent). They are divided into two categories: (1) continuous; and (2)
non-continuous lung sounds.
The program that I work at
utilizes the pulmonary nomenclature developed and adopted by the American
Thoracic Society and the American College of Chest Physicians, as published
in the Essentials of Cardiopulmonary Physical Therapy (3).
In this document, all continuous adventitious sounds are referred to as
wheezes and described as either high-pitched or low pitched. Wheezes represent
airway obstruction which can be caused by broncho-constriction of smooth
muscle or the presence of mucus. When a wheezes occur, it is significant.
They are most common with expiration. However, they can occur during inspiration
and this indicates that a severe airway obstruction is present.
Discontinuous adventitious
sounds are classified as either:
1. Crackles
sound like brief bursts of popping bubbles. They are most commonly associated
with the sudden opening of closed airways.
2. Pleural Rubs are
an indication of pleural inflammation and sounds like two pieces of sandpaper
rubbing together throughout each inspiration and expiration (3).
Exercise physiologists can become
proficient at auscultation by practicing on friends and family. There
are also numerous web site that offer auscultation tutorials. For example,
http://www.wilkes.med.ucla.edu/inex.htm
http://www.medinfo.ufl.edu/year1/bcs/clist/chest.html#AA11
Why is This Important?
Exercise physiologists work
in a variety of settings. The most common are clinics, fitness centers,
and businesses to name a few. They are asked to work with a variety of
people with a variety of conditions. I have been a practicing exercise
physiology for five years. In that time, my ability to auscultate has improved
a great deal. However, Ill never be as good as a physician and,
fortunately, I do not need to be. I do need to be able to use my physical
senses to assess how my patient or client is responding to exercise stress.
As an example, a 32-year-old
female presents at your gym. In her medical history, you notice she reports
asthma as a child. When questioned she states, I outgrew it and it doesnt
bother me anymore." Over several weeks at your facility, you notice that
she is disproportionately short of breath and frequently has coughing spells
with aerobic exercise. What do you think might be going on? It could be
that exercise is a trigger for her asthma. One way to provide her with
more information would be to auscultate when she is experiencing these
symptoms to see if she is wheezing. Will you diagnose asthma, No!
But you can provide her with information to report to her physician so
she can be treated possibly saving her life and retaining a member for
your facility.
References
1. ACSM
Resource Manual. (1998). (3rd Edition). Philadelphia, PA: Lippincott Williams
and Wilkins
2. R. L.
Wilkins, S.J. Krider and R. L (1995). Sheldon Clinical Assessment in Respiratory
Care. St. Louis: Mosby.
3. E. A.
Hillegas and H. S. Sadowsky. (1994). Essentials of Cardiopulmonary Physical
Therapy. Philadelphia, PA: W. B. Saunders Comapny.
4. Grays
H. (1901). Grays Anatomy. Philadelphia, PA: Running Press.
5. Tabers
Cyclopedic Medical Dictionary. (2001). (19th edition). Philadelphia, PA:
F. A. Davis Company.
6. Marieb
EN. (1988). Essentials of Human Anatomy and Physiology. Menlo Park, CA:
Benjamin-Cummings Company.
7. http://www.wilkes.med.ucla.edu/inex.htm
accessed 8/02/01.
Please forward any questions
and comments to the author at mkaelin@sirh.org
Copyright
©1997-2001 American Society of Exercise Physiologists. All Rights
Reserved.
ASEP
Table of Contents
Questions/comments
